bobh
-
Posts
340 -
Joined
-
Last visited
-
Days Won
20
Content Type
Profiles
Forums
Blogs
Store
Events
Everything posted by bobh
-
Praying it's PANS and not Pathological Demand Avoidance
bobh replied to Coutts75's topic in PANS / PANDAS (Lyme included)
Things are changing. A few years ago, in pretty much most countries, PANDAS would have been either not known (or, as in our case) it's existence outright denied. If you don't get a positive strep test and someone insists that therefore it can't be PANDAS, there is also PANS - virtually the same thing, but caused by other infection (or environmental trigger). There is still reluctance to accept the illness. Where I am, a doctor at a renowned children's hospital has said "I won't believe it is PANDAS unless there are two documented strep cases on file". But this is not the official definition (see the pandasppn or pandasnetwork sites) - a provisional diagnosis of strep can be given even if the child was known to be exposed to strep (at family or school). -
how do we treat my son if he can't leave my house?
bobh replied to tinaw's topic in PANS / PANDAS (Lyme included)
Some would call that low, but it's not necessarily low enough for PANDAS patients. Dr. Tanya Murphy found that more than 1/3 of 38 pandas patients reacted badly to that kind of dose, and only improved when starting at about 1/10th that dose. Here is her paper: https://www.researchgate.net/publication/228785018_Selective_serotonin_reuptake_inhibitor-induced_behavioral_activation_in_the_PANDAS_subtype We followed that advice and convinced our prescribing pediatrican to start at 2.5mg zoloft, and we had a dramatic improvement right away at that level (the pediatrician actually didn't believe it, because it was a sub-therapeutic dose, but the Dr. Murphy reports the same - improvement for some at really low levels, and sometimes really bad reactions at "normal low" levels) -
Yes, long post, but good - thanks. It is so encouraging to hear that your daughter is "worried about hair and makeup". I didn't think that I for one would ever say that, but after the catatonia, that is truly so good to hear. How did you get to the point of getting tociluzimab? I presume it was an immunologist that prescribed it. Your posts are the only ones that mention this drug on this forum (according to the search function, if it is working correctly), so this one is not well known, and maybe should be. Our son had catatonia-ish symptoms not long after his onset - usually once or twice a day, lasting from 10 minutes to just under an hour. We took videos, and a neurologist (that outright rejected PANDAS as not a real thing) pronounced them to be "psychogenic seizures". Wikipedia also defines catatonia as "a state of psychogenic motor immobility and behavioral abnormality manifested by stupor." I wonder if we should use a different word, because psychogenic (i.e. "of psychological origin") is definitely the wrong idea here.
-
Most Effectives Treatments for PANS/PANDAS
bobh replied to eacampbell67's topic in PANS / PANDAS (Lyme included)
I have finally gotten around to reading the 2nd link above. It seems to be a very exciting development for lyme treatment, but then it says "Direct extrapolation of these in vitro findings to human treatment would be unwise and premature." Has anyone had experience doing the 3 abx in combination anyway? -
Was the IVIG done for PANDAS/PANS? Who was the ordering doctor, if you don't mind me asking.
-
Pandas/Pans Testing for 5 year old
bobh replied to Kellbell98's topic in PANS / PANDAS (Lyme included)
We all want a definitive biomarker for PANDAS/PANS, but it is not to be had. The Cunningham Panel was never touted as a true biomarker, only as indicative - but even that is now in significant question (see below). Given that, a better choice for your money would be to book one of the top PANDAS/PANS experts that have had extensive case loads. Those experienced experts will know that strep blood work coming back low (when symptoms have been present for a very long time) does not necessarily mean no to PANS or PANDAS.
-
Anti-DNase B Strep high, but no treatment?
bobh replied to JSL25's topic in PANS / PANDAS (Lyme included)
There is a not-so-low false negative rate with swabs and cultures. If you do, say, 3 swabs in a row (on the same patient at about the same time) and 2 are negative and one positive, you should call it a positive, because the false negative rate is much higher than the false positive rate. (From this study: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2095077/ one can calculate the false negative rate as 28.1%, and the false positive rate as 5.7% - but that is just for that particular kit and the way it was used - results for other kits and techniques can vary). -
Yes, I have heard so - would take a bit to find out where I heard/read it. All I can find right now is a comment " In some of the US groups there have been discussion about other kinds of strep." (other than A).
-
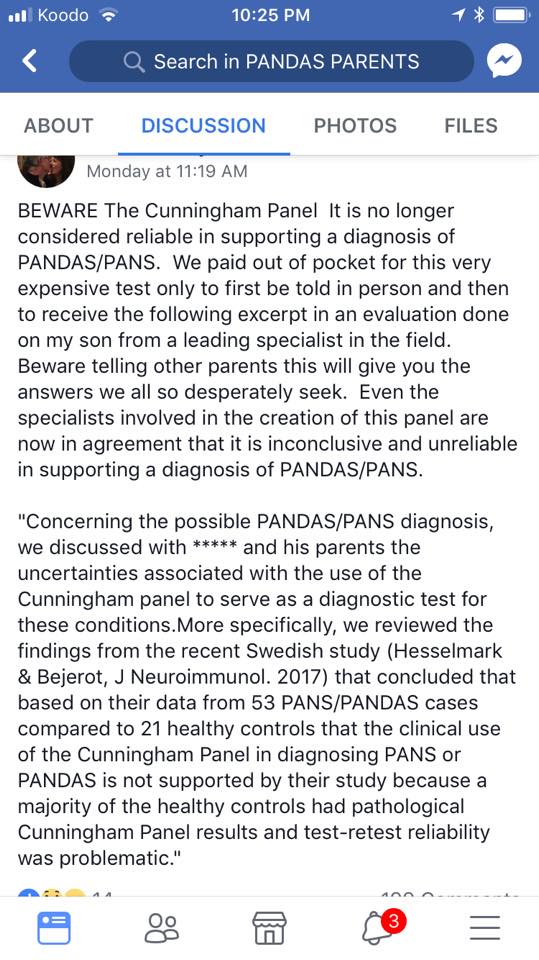
Ok. I would still suggest that if he is not well experienced in PANS/PANDAS, he may not get it right, even though he is otherwise very experienced, smart, etc. It is a strange and complex thing, and the experienced practitioners know that these particular boxes have been defined initially for research purposes, and then shaped by some strange politics, so that just because a person doesn't perfectly fit the box that has been defined, that doesn't have to mean "no" - the box could be a bit off. I was also surprised about that Cunningham panel - but I haven't read the Swedish study, or any rebuttals or criticisms of that study, if they exist yet. I certainly would if I was shelling out the money. This is another example of the importance of a "buyer beware" attitude - that it is best to educate yourself, if you have the capacity to get into it. My goodness, this is too much for a 17-year old, especially given that you are also struggling with symptoms. But you have come here, so you are already on the path. There is a lot of stuff on the www that you can read, but to give what you might stumble across about PANS/PANDAS some context, the documentary "My Kid Is Not Crazy" might be helpful (that will start to explain the "strange politics").
-
The attached is a post about the Cunningham Panel that came from another group. I always knew that it was not definitive, but this was a bit of a surprise. It may not be worth spending the money on it.
-
Most Effectives Treatments for PANS/PANDAS
bobh replied to eacampbell67's topic in PANS / PANDAS (Lyme included)
I would like to suggest that one "treatment option" is to not add too many things or make too many changes at once. These kids can react so individually and differently, and a "throw everything but the kitchen sink" strategy can result in a confounding "who know what is causing what" situation. For example, in some (rare?) cases, vitamin D makes some kids worse. That is even when they might be low on vitamin D in their blood - go figure (and some have went and figured, and have explanations for this kind of paradoxical thing). Somewhat less rare (in my humble opinion) but still rare, are kids that get worse on probiotics. Our son was measurably worse (I keep track of daily soap use as a measure of his OCD) on many different probiotics. Some kids react strongly to some probiotics, some parents mistake that (in my opinion) for herx, and some (such as my son) get mildly worse on probiotics. And of course, many have no problem with probiotics. But if you don't introduce them separately (i.e. have them on it for a week before abx), you won't know what is doing what. You can also try to figure that out by removing things later. There is more than one story of a mom that in desperation (when her child was not improving) took the child off everything - and the kid got better. But again, you won't know what was the culprit unless you remove one at a time, wait and watch, add back in, wait and watch, remove again, wait and watch, remove another, wait and watch, etc. It is a long road, and also a less-travelled path (because we can't be patient enough - we want a quick fix). -
Tough to call. You can search both here in this group and see comments that people have made before. I would think that Dr. T is more experienced with PANDAS, as he has had a very long history of cases.
-
I haven't worked with him, though I did hear him on Radio PANDAS some time back (you can find and listen if you like). You can also find a few comments (people here have asked about him before) at the following links: https://latitudes.org/forums/topic/21034-dr-horowitz-vs-dr-bock/ https://latitudes.org/forums/topic/20952-anyone-seeing-dr-kenneth-bock-in-ny/ https://latitudes.org/forums/topic/24938-dr-kenneth-bock/
-
I would recommend further detailed dissection of the "things are pointing towards a no for PANDAS/PANS". We have found some in the health care field "play along" with some tests and such, full well planning to say no regardless of results. Does your psychiatrist have a current PANS/PANDAS caseload of some size, i.e. an expert? I am coming from a place where I feel I have to "take over" and sift the evidence for myself, and make my own decision (to get a second, third or further doctor's opinion).
-
I was also surprised about a doctor advocating indefinite ibuprofen use. I hope that mountainmom can give us the link she was referring to, because I have not found it on either pandasnetwork.org or pandasppn. But I did find this paper that talks about long-term prophylactic use, maybe this is what she was referring to: http://online.liebertpub.com/doi/10.1089/cap.2016.0193 An important part of the question is dose. Some who have been doing short bursts of ibuprofen have also been doing higher and/or more frequent doses. But there are doses and times and liver checks all wrapped into the paper above, so even if it's not the research mountainmom meant, it looks like good solid info. Our kid didn't respond to ibuprofen, so I never pursued it. But I would be asking the same questions as you if it would have worked. Good luck!
-
I would say that even though you are fairly certain she has PANS and your pediatrician is not taking that seriously, because some of her current symptoms (diarrhea, nausea, pale) are not specific to PANS per se (as I understand it), you are best to take her in sooner and not wait. My own strategy with a non-PANS believing doctor in such a situation would be to be mum on PANS/PANDAS, and just let the pediatrician assess and treat what the symptoms that are presented. Your daughter could get treatment for something that could be important to catch earlier. Also, even with a "no mention of PANS" strategy, the doctor might do some tests that are helpful for PANS.
-
"I wanted to look into physical reasons first" - good for you. I do feel sorry for those that trust every word of a doctor as gospel truth, and give up on thinking. I agree with MomWithOCDSon - the timing of all these factors together (including the separation anxiety, which is a common symptom) are key here. It is very unlikely to be a co-incidence that these things just happened by chance together, without being tied together (by PANDAS). If you haven't already found http://www.pandasnetwork.org/ and https://www.pandasppn.org/ , spend some time there - these are solid resources backed by a stellar advisory panel. And to understand (at least partly) why some doctors refuse to acknowledge PANDAS (if that bothers you), you can check out the documentary My Kid is Not Crazy.
-
Praying it's PANS and not Pathological Demand Avoidance
bobh replied to Coutts75's topic in PANS / PANDAS (Lyme included)
There is so much, and some get overwhelmed by the volume of info (and who to trust). But those pandasnetwork and pandasppn sites are quite solid, which you can see by checking out their advisory boards (all the big names in PANS/PANDAS research and experience). Another item (if you are not too overwhelmed) is the documentary "My Kid is Not Crazy". If you are not aware of the controversy, this will be a head spinner. But it is also important to understand why some doctors dismiss PANDAS and PANS. -
Praying it's PANS and not Pathological Demand Avoidance
bobh replied to Coutts75's topic in PANS / PANDAS (Lyme included)
I am so sorry that no-one has responded to your post throughout this week. I have never heard of PDA, and a search in this group (including the full term Pathological Demand Avoidance) comes up with only your post. I think it would be wise to pursue the "PDA doesn't just appear" line of thinking and consider PANS/PANDAS. Unfortunately, 1 week of one abx may not be enough, especially with the cough/cold you reported. How was he later in the week? For more on abx protocol, have a look at http://www.pandasnetwork.org/understanding-pandaspans/antibiotics/, and also https://www.pandasppn.org/wp-content/uploads/PANDAS_Flow_Chart.pdf (which is actually a site to help doctors). -
Coming to terms, preventing flares
bobh replied to MountainMom's topic in PANS / PANDAS (Lyme included)
Our son was on non-prophylactic antibiotics (a variety of them) for about 2 years, but then in the spring of 2016, he progressively got worse while on them. We were frantic - something had to change, but we didn't know what. We decided to take him off abx (Ibuprofen had not helped him, and this was a long term progressive worsening). We eventually found out (after a teeth cleaning that produced a huge flare) that he had gingivitis, and when we dealt with that, we found some of the relief we were desperate for. While he was improving with the mouthwashes and more regular flossing/brushing that we implemented, we tried a supplement that a mom in a local group we belong to found repeatedly kept and took her daughter out of flares. I was intrigued when this mom reported that every time they ran out of this stuff and forgot to replace it in time, their daughter got worse. The supplement is phosphatidylcholine, and I was glad to discover it was well researched for all kinds of things, but not specifically for PANDAS/PANS. So, I had good documentation that it has been safely used at certain (higher than on the bottle) doses. I tried my child on the (high) dose the mom had settled on, and took him on and off it several times, while keeping track of his soap use (which we have found to be a reasonable objective measure of his OCD). The result was that his soap use was reduced (statistically significantly). So even though it didn't take all the OCD away, it helped reduce it. We have been on that for almost a year. I was surprised to see that phosphatidylcholine is not much discussed in this forum, but there were a couple of posts about it. I added my "research result" to one of those posts, here: http:// http://latitudes.org/forums/topic/18965-phosphatidylcholine/#comment-186762 . Another mom (in another group local to me) that tried phosphatidylcholine after we reported our results did not find an improvement. So, like most things (it seems), one size does not fit all, and this might not help your child. -
Uncontrollable yelling! Is it yeast flare?
bobh replied to xh1688's topic in PANS / PANDAS (Lyme included)
This brings up a very good point - how does one know whether a supplement is doing something good but causing a herx-like reaction, or whether it is itself causing a problem (i.e. the supplement is the toxin). This is a tricky question, but I do believe that the two can be teased apart. As an example, I have heard several people claim that probiotics caused a herx reaction in their child. I am a bit suspicious about that, because of the mechanism by which a probiotic would do that. I would understand it to (relatively slowly) crowd out other bacteria in the gut, so that the way you could potentially get a herx is 1) the current gut bacteria are bad, and flare-causing (an assumption that begs for validation) 2) the introduced probiotic gets a foothold and crowds out the bad stuff. But I don't think that works well. The probiotic doesn't directly kill the supposedly bad guys, it just takes their resources and either prevents them from growing more, or starves them (slowly, as the probiotic takes hold). That doesn't (to me) sound like a process that can send enough killed bad guys into the bloodstream (where the anti-bodies can pick them up and over-react) fast enough to do what we know as herx. If there is another mechanism, then I'm all ears. In my own case, my son was on a probiotic for over a year. When we stopped he got better. It couldn't have been a herx for a year. Then when we put him back on, he got worse. We did that two more times, each time off he was better, each time on he was worse. I concluded that was a bad reaction to the probiotic itself (i.e. it itself was toxin-like, for my kid). -
New to PANDAS and have a million questions
bobh replied to OhioDad's topic in PANS / PANDAS (Lyme included)
I understand this to work by crowding out the strep bacteria with something that is better for oral hygiene. I have tried the gum form as well, which I think it is a reasonable measure to consider for throat-discovered strep especially if it hangs on despite the abx. Mouthwash to kill everything you can, and then water rinse to get rid of residual mouthwash, and then the gum to replace the bad guys with better guys. Note that strep can exist in all kinds of other places (including inside the tonsils), for which the gum form of K12 blis would be useless. -
New to PANDAS and have a million questions
bobh replied to OhioDad's topic in PANS / PANDAS (Lyme included)
Welcome to the group. I would say you are very fortunate in how your circumstances lead you to rather rapid proper treatment. There are some who have struggled for very long, even years, and then discovered PANDAS. Your doctor may want to try to find out for herself if PANDAS is real - commendable (much better than taking another unbelieving "older experienced" doctor's word for it, which most seem to do, and which so keeps the truth from spreading). But, taking your daughter off the abx (at an early stage) to see if the symptoms come back is an experiment on your child that is not necessarily in her best interest in the very near term. If you need that kind of verification, then go for it - the experiment would be much more important in that case. I would think that a pandas specialist would be better because they won't need to do that experiment. But, if you want to further the cause and bring another skeptical doctor into the PANDAS fold for the greater good, well that could be another good reason (though for me, that idea is not free of ethical concerns). I think you got a good answer on the steroids. If your daughter gets to a state where symptoms spike even though on abx, try ibuprofen first (can't be on that long term, though). Seek out and watch the documentary "My Kid is not Crazy" (it is about PANDAS), for which you will need to fasten your emotional seat belt. There is still plenty of nasty controversy. -
Uncontrollable yelling! Is it yeast flare?
bobh replied to xh1688's topic in PANS / PANDAS (Lyme included)
I don't know that these symptoms you list (i.e. ramped-up PANS symptoms) are specific to yeast (i.e. I don't think that you can tell from the symptoms alone that this is from yeast). But I believe it is very possible. However, if the "more non-verbal yelling, talks less and ... tiny rashes" appeared relatively soon after starting the Japanese Knotweed and curcumin, I would first suspect those as the culprits - only because of the timing link. If that increase in symptoms started before those two items were added, then it can't be initially caused by them. As odd as it sounds, I gained most of my respect for supplements when I found out that some of them made my son worse. In some cases (not as rare as it should be), it could be because the supplement itself is not made to good standards, and is not all it is supposed to be (they are not regulated like drugs, so it is buyer beware). But in (I hope) most cases of reactions to supplements, it is probably just an individual reaction to something there that is otherwise ok for other people. I now try to introduce anything new by itself with no other known changes for several days, so I can tell if it might be causing a problem. This is not to say not to pursue the yeast route, but it is quite easy to take him off something and see if that makes a difference. As far as antibiotics and herbs combo, I use several of the many interaction checkers that are available, such as https://reference.medscape.com/drug-interactionchecker , https://www.drugs.com/drug_interactions.html , https://www.rxlist.com/drug-interaction-checker.htm and https://www.webmd.com/interaction-checker/default.htm . Use more than one - some list more supplements than others, and ideally you should get at least two saying the same thing (unless you really know and trust one of these websites). -
Coming to terms, preventing flares
bobh replied to MountainMom's topic in PANS / PANDAS (Lyme included)
Fantastic news! I am going to give an odd answer, and then answer the way I think you wanted. There is something PTSD-ish about having dealt with a PANS/PANDAS child for years. PTSD (Post Traumatic Stress Disorder) puts any normal person on edge about the possibility of being re-traumatized. That terrible reality is something that can be worked on and changed for the better - there are tips and tricks and techniques that a few lines of reply here cannot possibly do justice to. This is just encouragement to investigate that possibility (when you have a bit of a breather, like now), and it comes as much from personal experience as from your question. I think that it is realistic that you used the words "inevitable flare", even though that doesn't help the PTSD-ish issue. (It would be so much better for the next little while to be free from that fear. The fear is exaggerated, though - that's how it works.) I have found myself over time evolving through 2 stages, 1) investigating all possibilities of triggers (and there are so many) when a flare happens, and 2) after some years, recognizing that the thing has morphed into a more complex immune system thing that don't necessarily fit the simple trigger theory (or else, the triggers are so subtle, they can't be teased out. The good news about stage 2, is that the child (ours, anyway) is better - we are into the smaller flares, not like the horrors of the past, and they are by definition harder to figure out. We have only started this 2nd phase (if my thinking is even correct) in the last year or so. So, if my thinking is right and there is such as thing as the stage 1 I described, and you are in it, it's a long road of getting familiar with what sets your child off into a flare. Some of what we have learned is weird - like the time our son had a huge flare after a teeth cleaning. Those things are most efficient to figure out as you experience them. You can read in advance about various experiences here or in places you trust, but its a lot of reading. If you start reading around, take comfort that you can also get help from this and other groups when a flare happens. In the meantime, have abx and ibuprofen handy (unless you have figured out that ibuprofen doesn't work). Another place to do some reading, if you haven't visited, is pandasnetwork.org, in particular http://www.pandasnetwork.org/your.../post-traumatic-stress/ for help with coping as a parent.